Can my patient go home sooner?
Clinical decision support, from diagnosis to discharge, in your back pocket.
Take the History (Hx) and make the call.
Care can continue beyond hospital walls, at home.
Made for the clinicians who carry the decision.
From the ward round to the front door: risk scores, eligibility and the words for the referral, right where the decision happens. In your back pocket, on the device you already carry.
How we're different from other healthcare apps.
- ✓Show the guideline
- −No risk-score calculators
- −No eligibility logic
- −No referral or discharge text
- −No audit trail
- ✓Sit inside the EPR
- −Locked to one Trust
- −No portability for rotating staff
- −No social or transport prompts
- −Audit by EPR analyst only
- ✓Capture the conversation
- −Only after the decision
- −No pathway logic
- −No senior-review prompts
- −No referral routing
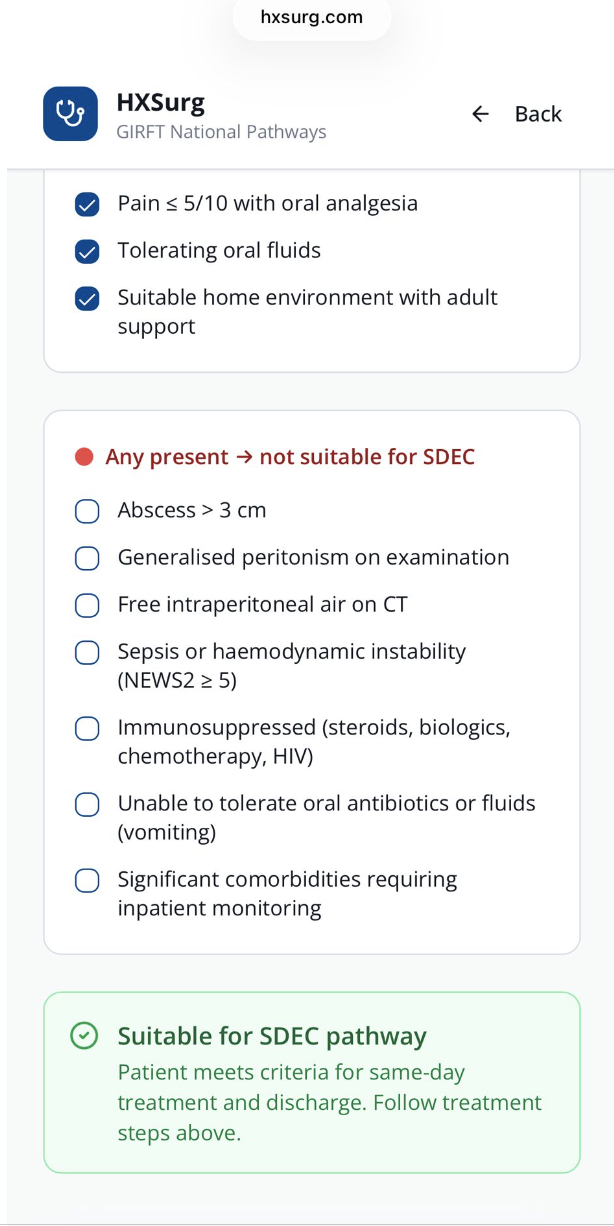
- ✓Risk scores at point of decision
- ✓Active eligibility & exclusion logic
- ✓Social, transport & home checks
- ✓Editable referral & discharge text
- ✓Anonymous audit: who, why, why not
A few extra referrals. Major savings for every Trust.
Just 10 additional appropriate H@H referrals per month could save a Trust £216,000 per year.
Every appropriate patient managed safely outside an acute bed releases capacity and reduces cost.
See calculation assumptions
- H@H / virtual ward bed-day: approximately £133 per day
- Acute hospital bed-day: approximately £600 per day
- Acute bed cost is therefore around 4–5× higher than H@H
- Estimated net saving per bed-day shifted from hospital to H@H: approximately £450
- 10 additional referrals per month × 4 avoided acute bed-days × 12 months = 480 acute bed-days released per year
- 480 bed-days × £450 net saving per bed-day = £216,000 estimated saving per Trust per year
Illustrative. National figure based on GIRFT General Surgery guidance on same-day emergency care and ambulatory pathways.
Built together with the NHS.
Royal United Hospitals Bath is our first pilot site. Strategic partner with Flexicare, domiciliary care providers. Supported by Health Innovation West of England.

 Domiciliary care
Domiciliary care
 HSJ Partnership Awards, Finalist
HSJ Partnership Awards, Finalist
Coming to a hospital near you.
-
2026 H1 · Now
First pilot at RUH Bath
Pancreatitis, diverticulitis, post-op robotic colorectal.
-
2026 H2
Scale across general surgery
Pathway expansion, configurable per Trust.
-
2027
Expand to other acute specialties
Acute medicine, cardiology, gynaecology, urology.
-
Beyond
From rules to learning
Anonymised decision data supporting smarter eligibility; clinician always in the loop.
We want to hear from you.
Whether you've used Hospital at Home, wish you could, or want to help shape the next pathway.
Bring HxSurg to your Trust.
Two minutes. We'll be in touch within 48 hours.